"And the waves went unknown where the pebbles shook under the shore. .."
"And the waves went unknown where the pebbles shook under the shore. .."
Benign paroxysmal positional vertigo( DPPG) is an equilibrium disorder that has, firstly, a transient, unstable character, and secondly, it is always due to a cause that does not representimmediate danger to life, because the disorder is called benign.
For the manifestation of pathology, it is necessary to occupy the body with a certain position. The position taken in the process of life involuntarily, or attached to the body specifically, with a diagnostic purpose.
And paroxysmal positional dizziness at least once in life experienced by everyone: the horizontal hitherto floor under your feet begins to slowly or quickly tip over to one side, or turns into a swing.
A bit of anatomy and physiology
What looks like a rocking of the picture before your eyes can be accompanied by a redistribution of the cerebrospinal fluid inside the brain cavities and perceived by the pressoreceptors of the nervous system, but not to be felt clearly.
For a direct perception of the position of the body in space, nature created a labyrinth.
This is a saccular formation in the cavity of the inner ear with three semi-circular channels oriented perpendicular to each other outgoing from it. The cavity of the whole complex is filled with endolymph - the origin is the same as the cerebrospinal fluid - and the "heart of the device" is a complex sensitive structure with the participation of "auditory stones" - otoliths, or statoliths.
"Auditory" they because the labyrinth is part of the ear. 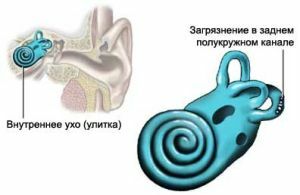
The otoliths, though small in their weight, exert a definite pressure on the receiving device of the analyzer of sense of equilibrium-a site of specialized nerve cells, the center of which is located in the large brain.
When the position of the body changes, the endolymph in the semicircles of the channels moves. When a current occurs in it, both the extension of a certain part of the organ occurs and the change in the degree of pressure of the otoliths to the "button" of the equilibrium analyzer.
Since the semicircular canals are three, we always know in which position we are: otoliths report the movement of the body up and down, right-left, forward-backward.
From the device of the receiver of the organ of equilibrium, the reasons for its failure, and the symptoms of the state that emanate from them, also flow out.
Mechanics of the disease and its causes
A "Christmas ball" helps to understand benign positional dizziness - when shaking, a "blizzard" of small bunches rises in the liquid filling it.
With DPPG, this state occurs when the position of the head changes or is shaken.
The otoliths in the field are reacting quickly and adequately to the "wave" that has arisen. But the otoliths break off form a suspension in the endolymph, first, thickening it and extending the time of the "wave", and secondly, distort the reflex.
 The most accessible for the accumulation of this kind of "trash" is the back channel( which is also vertical), which has the lowest bottom as with the horizontal position of the head, and with its vertical position.
The most accessible for the accumulation of this kind of "trash" is the back channel( which is also vertical), which has the lowest bottom as with the horizontal position of the head, and with its vertical position.
While the "snowstorm" is spinning from the otolith-debris, the manifestations of the syndrome are maximal, as the "garbage" subsides, everything stops.
In a large percentage of cases, the basis for the appearance of the phenomenon of otolithiasis - the accumulation of "fallen" otoliths-statoliths in the cavities of the labyrinth, has not been identified.
Causes that can cause benign paroxysmal positional vertigo:
- TBI( craniocerebral trauma);
- by viral labyrinthitis;
- by Ménière's disease;
- by the ototoxicity of medicines;
- with migraines on the NDC( with spasm of the labyrinth artery);
- by surgical operations on the ear or brain.
Symptoms with
Symptoms are expressed by sudden very intense paroxysmal dizziness with "swinging" of objects, either in the horizontal or in the vertical direction, or in one of the two. The cause of this symptomatology is always the change in the posture before the head and the problem ear of a certain position are taken, or the appearance of it due to a turn when turning in a cot, or due to the extension( bending) of the neck.
The onset of a fit of dizziness may occur when turning the head in a jerk, as in a sharp shout.
The seizure may have the character of a sense of uniform swinging, as in "seasickness", and can, like it, cause nausea.
Attacks are either single, or recur through equal time intervals, the frequency is from several a week to several in  for a day.
for a day.
The peculiarity is the shortness of the attack, the absence of a twisting of the head in an unchanging posture, as well as the absence of other concomitant symptoms in RAPP:
- of severe headache;
- deafness in the problem ear;
- noise in the ear.
Diagnosis of the disorder: samples, studies
The presence of the syndrome is checked using the Dix-Hallpike test.
The patient, sitting with his head turned at an angle of 45 ° towards the alleged pathology, is asked to fix a look at the point in the center of the person's face( on the nose).Then, holding it, it is sharply tipped over to the back, having thrown back the head at an angle of 30 ° with the same turning angle remaining in the problematic direction.
The test is considered positive if after a few( 1-5) seconds there is an attack of dizziness accompanied by a rotatory nystagmus oriented in the plane of the posterior semicircular canal. With left-sided lesion, the nystagmus coincides with the direction of the clockwise direction, with the right-hand one directed against its course. The time of nystagmus is within 30 seconds, not more.
After returning the patient to a sitting position, the nystagmus reappears, but the reversible one - in the direction opposite to the direction of the primary rotatory nystagmus, less pronounced and prolonged, accompanied by a slight dizziness.
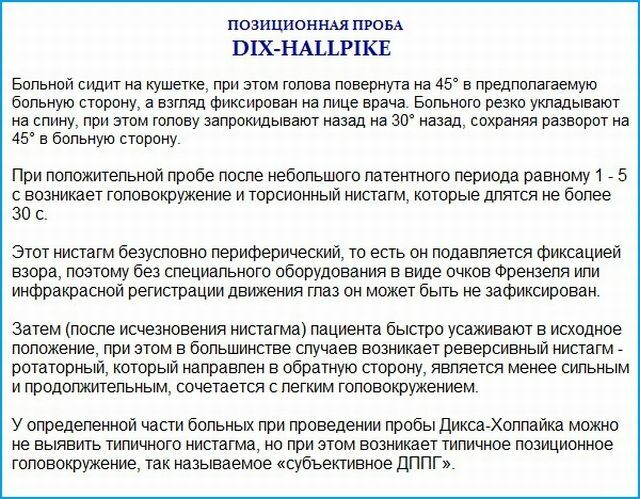
In case of doubtful results of the sample and in the absence of a typical nystagmus, they are guided by the appearance of a typical positional dizziness for this pathology.
For differentiation from a similar pathology, MRI( CT) scan of the brain, x-ray examination of the cervical spine, is applicable.
In addition to the use of neurological methods of research, it is necessary to involve other doctors in diagnosis: otoneurologist, ENT doctor, surdologist.
Treatment of BPHD - methods and exercises
The patient who understands the essence of the problem makes the correct conclusion: in order to avoid paroxysm, movements that shake otoliths with reaction from their receptors should be avoided.
However, to get rid of the patient from an unfortunate syndrome, in addition to the treatment of the underlying pathology that caused it, the technique of positional therapeutic maneuvers carried out with the help of a neurologist is used:
- Epley;
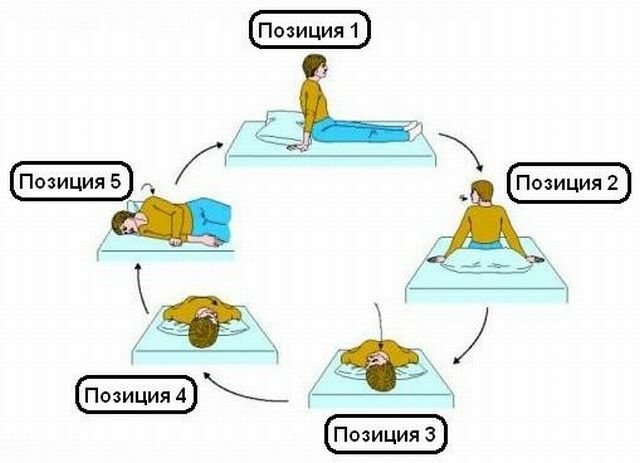
- of Brandt Daroff;
- Dismant or other authors.
Their essence consists in training the vestibular system by giving the head strictly consistent positions.
If necessary, microsurgical interventions are used on the inner ear with the filling of the affected semicircular canal with bone shavings or with the use of labyrinthectomy.
A photo-video compilation of the methods of treatment of DPPH: exercises by Brandt-Daroff, the maneuvers of Epley and Sonstort:
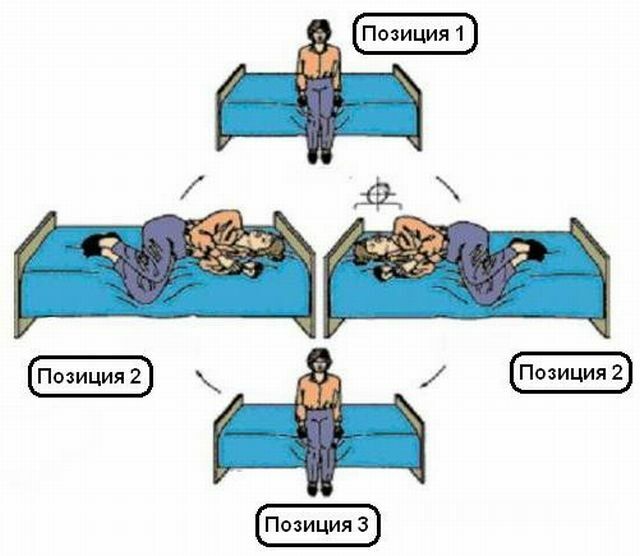
Brandt gymnastics
Maneuver Epley

Warn and not do harm
The following measures are used to prevent the development of PPPH:
- prevention of damage to the body of balance by viral and other contagious beginnings;
- caution when performing work and other vital functions;
- attentive attitude to the use of medicines;
- prevention of vascular disorders in the head and neck.
Prognosis depends on the degree of concomitant pathology. The disease can become dangerous when the patient is at a significant height or depth with the associated changes in atmospheric pressure, and also in the case of seizure in the control mechanism.