- Depressive stupor - occurs against a background of severe depression or manic-depressive psychosis. In this case, almost complete immobility of the patient, longing, a depressed expression, a hunched posture, a lowered look are characteristic. It is possible to give up food. Sometimes patients may show some reaction to questions, especially those given in a whisper. The attack of a depressive stupor lasts for a long time, sometimes up to several weeks, and in some cases can suddenly turn into a so-called melancholic rantus - a state of acute frenzy with autoaggression and craving for suicidal actions.
- Hysterical ( dissociative) stupor - occurs usually in emotional individuals with hysterical inclinations( much more often in women).The almost complete immobility of the patient with minimal reaction to external stimuli is typical. The patient often does not respond to questions, in rare cases can respond with a significant delay, short monosyllabic phrases. Spontaneous speech on its own initiative is absent, mental processes are slow and lack clarity.
- The hallucinatory - a state of stupor combined with auditory and visual hallucinations, which, in turn, cause the corresponding mimic reaction of the patient: joy, anger, fear, anxiety, surprise, etc. This kind of stupor is observed in organic psychoses, neurotoxic poisonings, and some forms of schizophrenia.
- Manic stupor - along with motor retardation and mutism, there are live mimicry, heightened mood and a certain interest in what is happening. Patients can follow the surroundings, smile for no apparent reason, weakly counteract passive movements under external influence. This type of stupor can occur with manic-depressive psychosis, but is currently rare because of the success in treating mania.

- Apathetic stupor - the patient usually lies on his back, is indifferent to what is happening around, inattentive to his appearance. He answers questions with a long delay, monosyllabic phrases. Muscular hypotension, sleep and appetite disorders are noted. Perhaps some manifestation of emotions in contact with relatives. This kind of stupor is observed with some long-lasting forms of psychosis, as well as with Wernicke's encephalopathy.
- Emotional( post-shock) stupor - occurs on the background of severe mental trauma( loss of a loved one, life threat), severe stressful situations( for example, soldiers in battle), accidents( fire, explosion, flood, earthquake) and other serious psychotrauma factors. With this kind of stupor, dulling of emotions and slowing of mental processes take place. Emotional stupor is more typical for women, its duration can be from several hours to several days. Often it passes independently, without treatment, but can go into a panic state or depression.
- Exogenous Stupor - occurs with toxic or infectious lesions of the subcortical structures of the brain, for example, in some forms of encephalitis or poisoning with neuroleptics. In its clinical picture, it is close to a catatonic stupor( see below), but it is isolated in a separate form, because with this type there is a clearly established cause of pathology and localization( subcortical nodes).
- Epileptic stupor - can develop against a background of epileptic psychoses, as well as after major epileptic seizures, especially serial. Often combined with frightening hallucinations and delirium. The depth of motor disorders in this type of stupor can be different - from slight inhibition to complete immobilization of the patient. The duration of the epileptic stupor is often short-ranging from a few minutes to an hour or a little more, but sometimes it can reach several days. In some cases, there is a sudden exit from the state of stupor, followed by an impulsive speech and motor excitement with aggressive actions.
- Negativistic stupor - characterized by complete immobility of the patient and resisting any attempts to change the position of the body. For example, the patient is very difficult to lay or sit, and then no less difficult to raise again on his feet( passive negativity).Sometimes a sick person, when trying to force him to act, performs the opposite action, for example, when he demands to open his eyes, squeezes them( active negativity).
- Cataleptic stupor( or stupor with waxy flexibility) - the patient for a long time( for hours and even days) keeps the externally imposed position, even if the pose is very uncomfortable( for example, with the raised leg and hand).The "air pillow symptom" is characteristic( the head raised above the pillow remains in this position for a very long time), sometimes it is a symptom of Pavlov( the patient does not answer the questions posed in a normal tone, but answers if asked in a whisper).Some patients show some activity at night: they can get up, move around, eat, answer questions, etc.
 The term stupor, meaning "stunned" or "stupefied" in Latin, means a pathological condition accompanied by a moderate impairment of consciousness, a decrease in patient orientation in the environment and a weakening of his reaction to all sorts of external irritations.
The term stupor, meaning "stunned" or "stupefied" in Latin, means a pathological condition accompanied by a moderate impairment of consciousness, a decrease in patient orientation in the environment and a weakening of his reaction to all sorts of external irritations.
The expression "to fall into a stupor" is quite common even in everyday life, meaning suddenly arose inhibition, disorientation, oppression.
If we talk about its purely medical significance, then it should be noted that the stupor states in resuscitation practice associated with somatic diseases differ from those that occur in psychiatry. These are qualitatively different states, but both of them fit into the definition of a stupor, that is, in both cases there is an oppression of consciousness with a decrease in orientation and inhibition of the reaction of the patient to stimuli.
Stupor-sopor-coma in resuscitation practice
In resuscitation, stupor is one of the urgent conditions with oppression of consciousness, preceding coexisting and coma.
Differences between stuporous, co-morbid and coma are manifested in the depth of the patient's disability:
- Stupor : drowsiness, impaired orientation in place and time. The condition resembles alcoholic intoxication, the reaction to external stimuli is reduced. The patient answers the questions slowly and sluggishly, often immediately falling asleep and falling into a stupor.
- : the patient is unconscious, only responds to strong stimuli( prick, shout, shaking), responding with targeted actions. The condition resembles a deep sleep.
- Superficial coma : a patient unconscious, responds to severe pain stimuli with random actions.
- Deep coma : the patient is unconscious, there is no reaction to any external stimuli.
Stupor, sopor or coma may occur due to a number of diseases, such as infections of the brain and its membranes, acute disorders of cerebral circulation, diabetes mellitus, liver and kidney disease, severe craniocerebral trauma, acute poisoning, drug overdose, alcohol,some medicines, etc.
Because of this, the state of stupor can occur in the practice of doctors of various specializations: neurologists, infectious diseases, endocrinologists, general practitioners, etc.
Stupor in psychiatry
Unlike the above, the various forms of the stopper that occur in psychiatry do not arise as a result of the general severe condition of the patient, but are a consequence of psychopathological processes and diseases. Stupor in psychiatry is seen as a motor impairment, consisting in inhibition of motor and speech activity, without any attempts on the part of the patient to overcome this condition.
Causes leading to this condition can be organic( schizophrenia, epilepsy, acute psychosis, intoxication, brain damage) or functional( stress, emotional shock, depression, prolonged fear, hysteria, apathy, etc.).
However, the specific biochemical and neurophysiological mechanisms of stupor have not been sufficiently studied to date. It is assumed that it can occur against the background of a deficiency of gamma-aminobutyric acid in the structures of the brain, with a sharp  deficiency in the body of dopamine and some other processes.
deficiency in the body of dopamine and some other processes.
Motor retardation in stupor can manifest itself in varying degrees - from moderate limitation in motion to complete immobility. Stupor is also characterized by mutism - a partial or complete absence of speech activity.
The patient does not attempt to get out of this state, and there is no willful direction in his actions. The duration of the stupor can range from a few minutes or hours to many months.
Types of stuporosis states of
There are many different forms of stuporous movement disorders in psychiatry, and they differ both in the causes of their appearance and in their clinical manifestations:

Catatonic stupor is the most common form of
The catotonic form of the stupor occurs most frequently and has several varieties, so it is worth dwelling on in more detail. The word catatonia itself comes from the Greek catatonos, which means "strained" or "tense".
Thus, catatonic is a stupor, in which motor and speech inhibition are accompanied by a significant muscular tension.
A similar kind of stupor is observed in schizophrenia and some psychoses. In severe cases of catatonic stupor, the patient does not make any attempts to commit any movements, he is completely immobile.
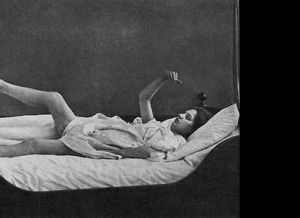
In the photo the patient who fell into the catatonic stupor
He does not try to react to pain and other irritations, to answer questions, shouting, etc. Such patients do not react to events around, all sorts of inconveniences, loud noises, bright light, wet clothing, dirt. They can remain immobile in explosions, fires, earthquakes and other extraordinary events.
There is no response to pain, including the Bumke symptom( dilated pupils with pain).Catatonic stupor is one of the manifestations of catatonic syndrome( along with catatonic excitation).There are three varieties of it: negativistic, cataleptic( stupor with waxy flexibility) and stupor with numbness.
Stupor with muscular numbness is the most severe form of catatonic, in which the maximum motor retardation is combined with the strongest muscle tension. Patients take the embryo pose and stay in it for a long time without the slightest movement. Often there is a symptom of the proboscis - the jaws are tightly closed, and the lips are extended forward. Speech activity is absent.
Forms of catatonic stupor can pass into each other, and also mutually replace with catatonic excitation. Their duration can be considerable - a person can be in a stupor from several hours( in light cases) to several weeks or even months.
Treatment of stuporosis states
Treatment of stupor should be performed in a hospital. In all cases, it necessarily takes place against the background of therapy of the underlying disease.
If the diagnosis is unclear, additional examinations may be required to clarify it( EEG, computed tomography, laboratory examinations, etc.).This is also important when there is a need to determine whether stupor is a result of somatic or mental illness.
Treatment of the underlying disease should be quite intense, taking into account the seriousness of this condition. At the same time, it is the prevention of relapses of stupor in the future. Of course, the spectrum of drugs may vary: for example, antipsychotics in the presence of schizophrenia, anticonvulsant with epilepsy, antidepressants in depression, etc.
With functional pathologies( hysteria, stress, neuroses, etc.), a good effect from psychotherapy is possible. 
Along with this, it is necessary to use drugs that disinhibit and stimulate the activity of the central nervous system. For this purpose, activating agents and psychostimulants( caffeine, Frenolone, Sydnocarb, etc.) are successfully used. As an additional therapy, it is appropriate to consider the appointment of nootropic drugs( Piracetam, Encephabol, Fentropil, etc.).
In a psychiatric hospital for the treatment of many types of stupor( catatonic, depressive, etc.) barbamyl-caffeine disinhibition is successfully used: intravenous injection of 1-2 ml of 20% caffeine solution, and after 3-5 minutes 5-10 ml5% solution of barbamyl. This method is also effective when patients refuse to eat.
When catatonic stupor is used also intramuscular injection of Frenolone in a dose of 5-15 mg per day. When the hallucinatory stupor  is used neuroleptics - Mazeptil, Triftazin, Haloperidol, etc. In the treatment of emotional, apathic, hysterical stupor, tranquilizers - diazepam, phenazepam, etc. can be used.
is used neuroleptics - Mazeptil, Triftazin, Haloperidol, etc. In the treatment of emotional, apathic, hysterical stupor, tranquilizers - diazepam, phenazepam, etc. can be used.
In general, the specific drug choice and dosage are determined by the attending physician, based on the form of the disease and the severity of the patient's condition.
Some of the possible complications of stupor have been mentioned above. In particular, emotional stupor can lead to the development of panic neurosis and depression.
Depressive, catatonic and epileptic forms of stupor can suddenly go into a state of arousal with aggressive actions against themselves and others. Stupor on the background of somatic diseases can be complicated by the transition to soporus and to whom.
Many of these conditions pose a threat not only to health, but also to the life of the patient, as well as dangerous to others, which makes intensive treatment activities with stupor mandatory.