
The inferior vena cava (IVC) is large retroperitoneal vessel, which is formed by the fusion of the left and right iliac veins. Anatomically, this usually occurs in the L5 region of the vertebra. The IVC is located in the right anterolateral side of the spinal column and passes through the tendon of the central diaphragm at the T8 vertebra.
Record content:
- 1 IVC Anatomy
- 2 Structure
- 3 Main functions
- 4 What doctors treat pathologies?
- 5 Possible diseases and symptoms
- 6 Diagnostic methods
-
7 Treatment
- 7.1 Surgical methods
- 7.2 Drug treatment
- 8 Video about the inferior vena cava
IVC Anatomy
The IVC is a large blood vessel responsible for transporting deoxygenated blood from the lower extremities and abdomen back to the right atrium of the heart. It has the largest diameter of the venous system and is a thin-walled vessel.
Other veins contain one-way valves that allow blood to flow directly back to the heart. Direct delivery to the heart is provided by the differential pressure generated by normal breathing.
As the diaphragm contracts and creates negative pressure in the chest to fill lungs with air, this pressure gradient pulls venous blood from the abdominal to the thoracic IVC, and then to the right sections hearts.
The inferior vena cava is located in the right atrial system of the heart. After passing through the diaphragmatic region, it enters the posterior inferior part of the atrium. Then it flows into the right atrium below the entrance to the vena cava of the upper part of the system (SVC). These anatomical characteristics make it ideal for transporting large amounts of venous blood.
Structure
Due to the fact that the IVC is located on the right side of the spinal column, the vessels entering the IVC on the left side of the body, like the renal vein, are longer than their anatomical counterparts on the right. Other veins on the left, such as the left adrenal and gonadal, first join the left renal vein, and then adjoin the inferior vena cava, and continue their venous flow, returning to heart.
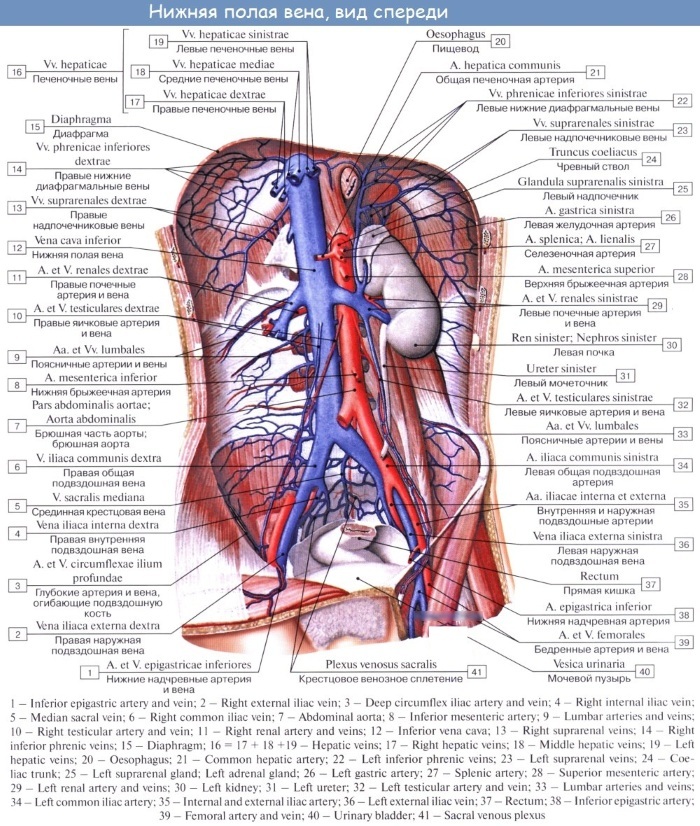
This structure differs from the right side of the body, where the adrenal gland and right gonadal vein are directly connected to the IVC without first connecting to the right renal vein.
There are different anatomical variants of venous anatomy involving both the right and left sides:
- Blood from the left and right femoral veins enters the IVC through the corresponding common iliac veins.
- Blood from the internal organs of the abdominal cavity enters the portal vein and then into the IVC through the hepatic vessels after passing through the liver and its sinusoids.
- Venous blood from the abdominal wall reaches the IVC through the lumbar veins.
- The ascending lumbar veins connect the lumbar to the non-permanent vein, which allows some collateral circulation between the inferior and superior vena cava.
This potential for side flow can be critical if any of the larger veins become blocked. Below are the data of the (most common) vertebral levels, on which different veins enter the IVC:
| Levels | Veins |
| T8 | Hepatic veins, lower phrenic veins |
| L1 | Right adrenal vein, renal veins |
| L2 | Right gonadal vein |
| L1-L4 | Lumbar vertebral veins |
| L5 | Right and left common iliac veins |

The inferior vena cava is ultimately responsible for transporting nearly all venous blood (deoxygenated) from the abdomen and lower extremities back to the right side of the heart for oxygenation.
Main functions
The inferior vena cava is located to the right of the midline of the drainage inflow. Its function is to transport blood from the abdominal cavity, pelvis and lower extremities to the right atrium of the heart. Additional IVC functions are seen in certain health conditions, such as obstruction of the hepatic portal vein or obstruction of the IVC itself.
Specialized vessels called portocaval (portosystemic) anastomoses open when the liver portal vein is blocked. The intestinal blood then bypasses the liver and goes directly to the IVC. In cases where the vena cava is occluded, the collateral vessels of the superior vena cava open, having time to engage adjacent blood vessels:
| The main function of the vena cava | The vein that collects deoxygenated blood from the abdomen, pelvis and lower extremities and carries it to the right atrium of the heart. |
| Source | Common iliac veins (L5) |
| Tributaries | Lower Phrenic, right Suprarenal, Renal, right Testicular (gonads), Lumbar, common Iliac and Hepatic veins. Mnemonic: passage through the liver and its tributaries |
| Clinical picture | Inferior vena cava thrombosis |

Anatomical variants of IVC are not common, but it is important to be aware of their presence and comorbidities / other common coexisting abnormalities. Unrepaired IVC injury, whether iatrogenic or traumatic, results in rapid exsanguination.
What doctors treat pathologies?
Vascular surgeons are highly qualified specialists in the treatment of diseases of the vascular system. All blood vessels - the arteries through which oxygen-rich blood flows and the veins through which blood returns to the heart - are the highways of the circulatory system.
Conditions such as hardened arteries can create "plugs" in the circulatory system, preventing flow to any part of the body.
A vascular surgeon can perform any surgical procedure:
- Some specialists specialize in 1 or 2 types of vascular interventions.
- They are mainly involved in open complex surgery and minimally invasive endovascular surgery.
- Vascular surgeons work with veins and arteries in all parts of the body except the brain and heart.
- They treat problems with the aorta (large main artery) after it leaves the heart and into the abdomen.
- Peripheral vascular disease, which often affects the arteries of the legs and feet, is also treated by a vascular surgeon.
Typically, patients are referred to a vascular surgeon by their physician.
Possible diseases and symptoms
There are many physiological options for IVC:
- Compared to the arterial system, the venous system is much more susceptible to congenital malformations, many of which remain asymptomatic throughout a person's life.
- If symptoms are present, they are often vague, and include only abdominal or lower back pain.
Some of the most clinically relevant physiological variants are listed below:
| Left inferior vena cava | The anomaly in it is caused by the regression of the right supracardinal vein with the preservation of the left one. |
| Education | The left inferior vena cava connects to the left renal vein and then crosses the anterior aorta before joining the right atrium to form the normal prerenal IVC. |
| Research frequency | The estimated prevalence of this anomaly is between 0.2% and 0.5%. |
| Double inferior vena cava |
 This anomaly is caused by the persistence of both the left and right supracardinal veins. The prevalence is assumed to be between 0.2% and 0.3%. This anomaly is caused by the persistence of both the left and right supracardinal veins. The prevalence is assumed to be between 0.2% and 0.3%. |
| Intrahepatic inferior vena cava agenesis | Congenital anomaly resulting in the absence of intrahepatic IVC. The intrahepatic venous blood supply bypasses the hepatic IVC through the nonsygotic / hemizygous venous system. |
| Absence of infrarenal inferior vena cava | This is the rarest of the physiological abnormalities of the hollow system. The putative and currently accepted etiology of the absence of the infrarenal inferior vena cava is intrauterine or perinatal thrombosis and, as a consequence, the degeneration of the infrarenal lower vena cava. |
The inferior vena cava can cause abnormal blood circulation in the chest or abdominal cavity. Since it is located at the junction of the plexus of all arteries, it is worth studying pathologies on the part of the respiratory and digestive organs. The principles of recovery from IVC damage are similar to other vascular injuries.
Although there are different methods depending on the site of injury and the experience of the surgeon, the primary goal is proximal and distal control of the IVC followed by a type of recovery. In a life-threatening situation, IVC ligation is successfully performed.
Although there is some disagreement about the indications, recurrent deep vein thrombosis and subsequent pulmonary embolism resistant to anticoagulant treatment may require the installation of a lower vena cava.
Some institutions are also advocating the installation of an IVC filter for patients with high-risk injuries (even without documented clots). Filters can be persistent or retrievable, although the data shows that only a subset of chunks are later removed.
Anatomical deviations from the norm require careful attention to details and an understanding of their manifestations, as well as possible complications during the procedures:
- IVC thrombosis is a complex clinical scenario. Although it may be asymptomatic, IVC thrombosis can present with many symptoms. They are usually nonspecific, such as abdominal or back pain.
- Treatment is based on the study of the patient's symptoms. This includes removing the anticoagulation, clot, and / or filter (if any) using interventional radiology techniques.
- Open surgical techniques are rarely performed. The most common cause of IVC thrombosis in a patient without anatomical symptoms is a previous insertion of an IVC filter.
Possible causes of CAP syndrome may indicate the development of oncology:
- Primary or metastatic cancer in the upper lobe of the right lung may compress the vena cava.
- Lymphoma or other tumors located in the mediastinum can also cause compression.
- Less commonly, the vena cava can be clogged with a thrombus from the inside. As patients undergo all invasive medical procedures, the symptom of IVC syndrome is found with increasing frequency.
- The blood clot (thrombus) that causes the disease is a complication of pacemaker wires, dialysis, and other intravenous catheters that are inserted into the inferior vena cava.
Historically, infections (syphilis and tuberculosis) have been another cause of IVS syndrome in other parts of the world. Sarcoidosis (a disease that results in a mass of inflamed tissue) can also cause this syndrome.
Diagnostic methods
The inferior vena cava is located in the atrium, therefore, first of all, radionuclide venography can be performed as a diagnosis. Contrast inferior venacavogram shows that the patient may have permanent right and left supracardia (double inferior vena cava), iliac vein occlusion with ascending lumbar collateral blood circulation.
Depending on the results of the study, other diagnostic tests may additionally be carried out: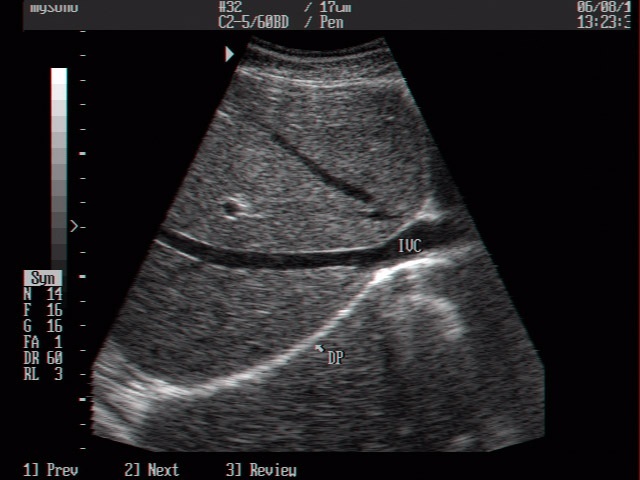
| Diagnostic method | Description |
| Retrospective and prospective studies | Include measurement of either the IVC expiratory diameter or the H-value subsidence index (IVC-CI). |
| Histological analysis | Conducted freelance if the clinical course of ADS is an absolute emergency. Irradiation can be started immediately. |
| Chest x-ray | An additional diagnostic method for detecting the presence of expandable metal stents. |
| CT scan | Performed if there is a suspicion of obstruction of the genital vein |
| Chemotherapy | It is used for high-grade lymphomas, germ cell tumors and small cell lung cancer because it is more effective than radiation therapy. For those who are less sensitive to chemotherapy, radiation therapy is the main treatment. |
| Sonographic assessment of IVC diameter | It can be used as a fast, simple, inexpensive, non-complicating, and reproducible method for differentiating cardiac and pulmonary causes of dyspnea. |
| Measurement in B-mode "i" | Performed to differentiate dyspnea in comparison with other diameters and IVC calculations. |
Successful experience with thrombolytic agents has been limited to the treatment of catheter-induced SVCS. Surgical resection of tumors associated with SVCS does not improve survival and should be avoided.
Treatment
Inferior vena cava syndrome is rarely a medical emergency. The ABC of Nursing is always a priority, ensuring that treatment can be adequate based on the tests taken and performed.
Most often, surgeons prescribe the following:
- Furosemide (Lasix) is a diuretic that reduces the amount of fluid in the bloodstream.
- Radiation treatment - is carried out only for 10% of patients with lung cancer who live with the disease for less than 30 months.
- Steroids - methylprednisolone (Medrol, Depo-Medrol) or prednisone (Deltasone, Liquid Pred) may be considered to reduce swelling of the tumor pressing on the inferior vena cava and relieve symptoms.
- Anticoagulant therapy - Warfarin or Coumadin is given.
- Thrombolytic drugs - alteplases (Activase, TPA, or TNK) to break a clot or place a stent to keep the vein open.
In children, inferior vena cava syndrome is most commonly caused by non-Hodgkin's lymphoma. The compression can also be associated with curvature of the trachea. In children, it is relatively narrow, flexible and soft, so airway obstruction can manifest itself as stridor, shortness of breath, and wheezing.
Surgical methods
People with STAI do not always need immediate treatment. This will depend on how severe the symptoms are, whether their airways are blocked, and whether blood is flowing well through other veins.
The inferior vena cava is located in the region of the heart, therefore, the DIME methodology (wound care, infection control, moisture balance and preparation of the wound margin) is used for treatment.
It is used as the basis for linking venous wound care products with their clinical effects. The doctor may prescribe corticosteroids to reduce swelling or diuretics to surgically remove excess fluid from the body by increasing urination.
If the syndrome is caused by a blood clot, the surgeon performs thrombolysis - treatment to break the clot inside a vein or place a stent to keep the blocked vein open. Surgery to remove any blockages can also be considered an alternative.
Drug treatment
When surgery is not required, medication is prescribed. In this case, it is important to take into account the routes of drug delivery to the middle segment of the inferior vena cava.
The best solutions are prescribing the following drugs:
- Norepinephrine (1-3 mcg / kg), injected into the right femoral vein, will cause a two-stage increase in tension in the middle segment of the inferior vena cava.
- The effect of norepinephrine is enhanced by the administration of cocaine in the amount of (2 × 10 (-5) M) in the same way.
- Acetylcholine (3 μg / kg) injected into the femoral vein results in a one-step increase in tension. If the drug is injected into the aortic arch, the vein contracts faster, but there is a risk of hypertension.
Within 3 months. the patient must constantly visit the vascular surgeon and undergo diagnostics. Thus, the dynamics of the clinical picture will be fully studied, and the patient will be able to recover by the end of the 2nd month.
The inferior vena cava is responsible for the delivery of blood through the circulatory system. When a disease is detected, a person may experience dizziness, spasms, and nausea. When diagnosing, the prerequisites for symptoms are identified, which facilitates further treatment of complications. The IVC is located at the confluence of the right and left iliac veins, passing through the diaphragm and mediastinum.
If there are symptoms of a disease that are not related to the blood vessels, the doctor may order a complete blood count and X-ray to understand how the organs function.
Video about the inferior vena cava
Inferior vena cava:


